Departments
Clinical Treatment Options
Jan 2008 —
Vol. 2,
Iss. 1
Self-Etching Resin Adhesives
Howard E. Strassler, DMD
Howard E. Strassler, DMD
The Holy Grail for adhesion to enamel and dentin has
been described as being a single
component, no-mix adhesive that can be applied directly to enamel and
dentin for the purpose of bonding any restorative material to tooth
structure. While this product does not yet exist, the manufacturers and
researchers are hard at work developing and evaluating improved bonding
systems. The introduction of self-etch adhesive systems has been an
important step in achieving this goal of an all-in-one bonding agent.
The idea of adhesive bonding to dentin was postulated
more than 50 years ago as involving a potential chemical bond between
the methacrylate group of resins to the collagen surface of dentin.1 In 1955, Buonocore
described a clinical technique that used a diluted phosphoric acid to etch
the enamel surface and provide for retention of unfilled, self-cured
acrylic resins.2 The resin would mechanically lock to the microscopically
roughened enamel surface, forming small "tags" as it flowed
into the 10-µm to 40-µm deep enamel microporosities and
then polymerized. The first clinical use of
this technique was the placement of sealants.3 The combination of
acid-etching enamel and adhesive composite resin restorations
afforded the benefits of reduction or elimination of microleakage at the
enamel margins, less discoloration at the margins, lower rates of recurrent
caries, and improved retention of the restoration.4,5
The effectiveness and success of the etched
enamel/resin bond has been demonstrated in many reported clinical trials.6 Unlike enamel
bonding, dentin bonding has seen an evolution in its viability. Effective
dentin-bonding materials should fulfill the following goals:
• The material should be retentive to dentin at a
clinically acceptable level, and should be
able to withstand intraoral forces of occlusion and mastication.
• The bond should be instantaneous once the
material has set.
• The material and technique must be
biocompatible.
• The material should
resist the forces of polymerization shrinkage
of composite resins and the coefficient of thermal expansion and contraction to eliminate microleakage.
• The material should create a long-lasting bond
to dentin.
• Postoperative sensitivity must be minimized or
eliminated.
In 1956, the earliest research with dentin bonding
focused on chemical adhesion of resins to the inorganic components of
dentin. Buonocore and coworkers developed a methacrylate-based dentin
adhesive that contained phosphate groups to attach to the calcium ions on
the dentin surface.7 The basis of the bond was the presence of the dentin smear
layer.8
While a weak bond was created, unfortunately it
was a clinically unacceptable bond to dentin. This basis of a
phosphate-calcium bond later became the third-generation phosphate-ester
bonding systems. These bonding systems, eg, the
original Scotchbond (3M ESPE, St. Paul, MN) and BondLite (Sybron Dental
Specialties, Inc, Orange, CA) among others, bonded to the calcium-rich
dentin smear layer and to etched enamel. Their bond strengths to dentin
were limited by the bond of the smear layer to the dentin. Unfortunately,
the durability of the bond was impacted by hydrolysis that occurred over
time to the phosphate/calcium bond.9,10 These products had limited success and the search for
a better adhesive to dentin continued.
At the same time, another research path for dentin
bonding investigated the use of a total-etch approach, etching the enamel
and dentin simultaneously.11,12 At the time, there was concern that phosphoric acid placed
on dentin would cause pulpal inflammation and necrosis.13 Jennings and Ranly
demonstrated that the pulpal effect of phosphoric acid on dentin for 1
minute was minimal.14 Early results reported on dentin etching were disappointing because the adhesive resin used was the
same unfilled, hydrophobic Bis-GMA bonding resin used for etched
enamel.12 The hydrophobic resin would not wet the moist, vital dentin and predictable adhesion could not be produced. The breakthrough in the total-etch approach was first described
in the late 1970s by Fusayama and coworkers,15
Bertolotti,16 and Kanca.17 They demonstrated the success of the total-etch adhesive bond based on the addition of a hydrophilic monomer, usually hydroxyethyl methylmethacrylate to the primer
and adhesive. This monomer allows the adhesive resin to penetrate the
peritubular dentin and dentinal tubules.18
These concepts led to the development of multi-step
adhesive bonding systems, which required the application of a primer
and then an adhesive resin, in the late 1980s and early 1990s that used a total-etch technique with phosphoric acid. In
the mid 1990s
clinicians sought a simplified approach that used fewer steps for adhesive placement. Manufacturers responded with the
introduction of single-bottle primer/adhesive total-etch bonding systems. With these two different classes of bonding
systems came the classification and description
of bonding systems based on generational timeline changes.
Fourth-generation bonding systems referred to total-etch, multi-bottle
(multi-step) systems and fifth-generation systems were total-etch,
single-bottle bonding agents that contained both primer and adhesive. Both
fourth- and fifth-generation products required a total-etch with phosphoric
acid before adhesive placement.
Simplification of technique and a reduction in the
number of steps was desired. It was obvious that the more steps that were required to bond a
restoration, the greater the potential for inconsistency in the
timing of application, rinsing, drying, rewetting dentin, and maintaining a controlled operative field
during treatment. This inconsistency has an
impact on the success
of the bond and the durability of the restoration. Manufacturers responded by placing research efforts in the
development of self-etching adhesive systems.1
Many manufacturers have referred to self-etch
adhesives as either sixth- or seventh-generation adhesive systems. In this
authors view, the description of adhesives based on a generational
view can be confusing. Christensen described a classification system for
bonding agents based on the components used to achieve adhesion to dentin
and enamel.19 He divided adhesives into two main categoriestotal-etch
(TE) and self-etch (SE). Within each category he then subdivided the
classifications based on the number of reagents that were used for the
adhesive technique. This classification system is listed in Table 1 with
examples in each classification. Table 2 lists recommendations for the
clinical applications of the two types of adhesive systems listed based on
the clinical evidence.
Currently, the clinician has the choice between two
different approaches for bonding that have different mechanisms in how they
interact with the dentin smear layer: a TE approach or a SE approach.20 The TE technique uses 30% to 40% phosphoric acid, which removes the dentin smear layer. The phosphoric
acid is rinsed with water and dried from the
dentin. The dentin is then rewetted with water,
leaving a damp surface; an adhesive resin is then applied.
The introduction of a SE adhesive simplifies the
bonding process. The SE approach does not
require a separate etching step because the etchant is incorporated into
the adhesive (either in a separate self-etching
primer or in the adhesive itself). Also, a
separate step of rewetting with water is eliminated because SE adhesives
contain water and are never completely dried from the tooth. SE adhesives
do not remove the smear layer but incorporate
it into the adhesive. Their compositions are
aqueous mixtures of acidic functional monomers, usually phosphoric acid esters, with a pH value higher than phosphoric acid (TE type) gels.21 It has been reported that the pH of Clearfil® SE Bond (Kuraray
America, Inc, New York, NY) is approximately
2.0, compared to a pH of 0.5 to 1.0 for typical phosphoric acid gels.22
SELF-ETCHING ADHESIVES
As stated previously, there has always been concern
for contamination and inconsistency with multiple-step bonding systems. In
response to this concern, self-etching adhesive systems have been
developed. Recent research has investigated self-etching adhesive systems.
A chief complaint among practitioners with composite resin restorations has
been the rate of postoperative sensitivity especially when using TE bonding
after the placement of Class 1, 2, and 5 restorations. Several different
studies evaluated postoperative sensitivity using both TE and SE adhesives.19,23-26 The results of these studies
demonstrated no difference in postoperative sensitivity between a TE and SE
adhesive. In fact, the conclusion of one study stated that postoperative
sensitivity may depend on the restorative
technique and variability among operators rather
than on the type of enamel-dentin adhesive used.19 This variability between
operators can be minimized by simplifying the technique of
adhesive placement with a SE bonding system.27,28 Table 3 lists the advantages of the SE bonding systems.
Other research has compared SE systems to TE systems.
Santini and coworkers investigated microleakage around Class 5 restorations
bonded with TE and SE adhesives.29 They concluded that SE systems
were as reliable as TE systems. One area of inconsistency with TE bonding
has been the bonding potential to
desiccated dentin.30,31 The inherent nature of SE
adhesives is no-rinse, leaving the surface moist. This may contribute to minimizing postoperative sensitivity.28 Finger and Tani investigated the effect of dentin wetness on bond
reliability and found that the SE adhesives were unaffected by relative
humidity of the dentin.32
Some clinicians are concerned about bacterial
contamination of cavity preparations and use cavity disinfectants before
applying dental adhesives. The use of benzalkonium chloride and chlorhexidine gluconate has been found to have no
detrimental effects on the sealing ability of no-rinse self-etching
adhesives.33 In some cases the self-etching adhesive acts as its own disinfectant. Both iBond (Heraeus Kulzer, Inc, Armonk, NY)
and Clearfil® Protect Bond (Kuraray America, Inc) have data to support this claim. With the increased interest in tooth
whitening and the availability of over-the-counter peroxide-based products,
the clinician may not know if their patient is bleaching their teeth.
Research supports waiting at least 1 week after bleaching before any
restorative procedure with either an SE or TE
adhesive to allow the enamel and dentin to recover from the bleaching procedure.34 It is
important to know whether or not your patients are using peroxide
products before any bonding procedure.
There has also been concern about the bonding quality
of SE adhesives to enamel. If enamel is left unprepared, it is resistant to
etching and adhesion with most SE adhesives.35-37
Bonding to unprepared enamel with
orthodontic brackets using SE adhesives has been reported. One study
demonstrated no difference in bracket retention between TE and SE38 while two other
studies had significantly more bond failures with the SE system.39,40 Clearly, there
are differences between SE systems when bonding to enamel. Multi-step SE
systems appear to be more aggressive in etching enamel.41-43 One study recommended
doubling the conditioning time with a SE system to increase bond strength.44 Clinical Research
Associates evaluated and compared TE to SE adhesives.45 They concluded that both
adhesives have similar bond strengths to prepared enamel and dentin. When
using any SE adhesive, it is recommended that enamel and dentin be prepared
with either a rotary diamond or bur. Prepared enamel and dentin will have
comparable bonding between TE and SE systems.45-48 Some concern has been expressed that a thick dentin smear
layer may interfere with bonding using an SE adhesive. Tani and Finger
demonstrated effective bonding with SE adhesives to thick dentin smear
layers.49
What is the evidence in clinical trials for the use of
self-etch adhesive systems? In recent years clinical trials using SE
adhesives have been reported at both the International Association of
Dental Research and American Association of Dental Research meetings. In
many cases at these meetings, the clinical trials reported as abstracts
with supporting documentation via oral presentations and/or poster
presentations may not be submitted for publication in dental journals. A
review of the last four meetings in Honolulu, Hawaii (2004); Baltimore,
Maryland (2005); Orlando, Florida (2006) and Brisbane, Australia (2006)
provided insight into a number of ongoing trials.
The clinical success of SE adhesives can be measured
in a variety of ways. In the cases of routine Class 1 and Class 2
preparations, retention is not a primary evaluation criterion for a
short-term study, but sensitivity and marginal staining are. For the
restoration of noncarious cervical lesions (NCCL), retention and marginal
staining are the benchmarks for success of an
adhesive system. In a 10-year study with the SE adhesive Clearfil® Liner Bond 2 (Kuraray America, Inc) Class 1 through Class 5 restorations were evaluated. At the 10-year recall,
90.9% of the restorations exhibited some marginal breakdown and 88.6% of
the restorations had marginal staining. The retention rate of the
restorations for those prepared cavity preparations and restorations with
the SE was 100% at each recall period (50.5% at 10 years or the original
placed restorations). This SE system was an
acceptable adhesive for restoring prepared teeth.50 Swift and coworkers
compared a TE (Optibond® Solo Plus, Kerr Corporation, Orange, CA) to a SE
(Xeno® III, DENTSPLY Caulk, Milford,
DE) for sensitivity and found that for both
adhesives, 23% of the treated teeth had short-duration sensitivity to
biting pressure that resolved after 10 days.51 A 24-month clinical trial with a two-step SE (Clearfil
Protect Bond) and a one-step SE (Xeno III) for
NCCL demonstrated retention rates of over 96%
with no postoperative sensitivity at the 2-year recall. Compared to 3% of
the Clearfil Protect Bond, 12% of the Xeno III restorations had marginal
staining.52 In an 18-month study with Clearfil SE Bond, enamel beveling or acid-etching did not improve the retention rate of NCCL restored lesions. The retention rate for the four groups
tested was 100%.53 A 5-year clinical evaluation of One-Up Bond F Plus (J. Morita
USA, Inc, Irvine, CA) with 42.5% of the original restorations recalled
showed a 92% retention rate, with 48% of the restorations demonstrating
marginal staining.54 Other studies have demonstrated similar results with SE
systems to those previously cited.55-63 Retention with SE adhesive systems is not a problem and
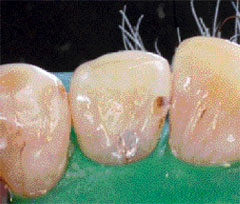
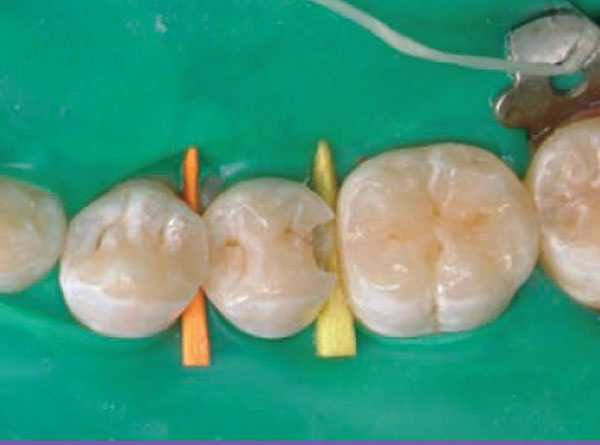
there are minor rates of marginal staining. Figure 1A View Figure ; Figure 1B View Figure; Figure 2C DI200801_59x.jpg
demonstrate two cases restored using SE adhesive systems.
An area of recent investigation has been the
compatibility of TE and SE systems with composite resin cementation. There
is contradictory evidence that some single-bottle adhesive systems do not bond well to self-cure and dual-cure composite resins
because of the acidity of the
single-bottle primer-adhesive. Studies
demonstrating a decreased bond and other studies showing no effect have been reported.64-66 Some recent studies evaluating SE systems and compatibility with dual-cure and self-cure composite resins have demonstrated some changes in
chemistry that have resulted in composite resinadhesive
incompatibility.67,68 This variance requires that the clinician review the manufacturers recommendations for use with self-cure and
dual-cure
composite resins.
CONCLUSION
Clinicians have seen multiple generations of adhesive
systems in the last 20 years. Many of these
bonding systems have required multiple
steps to include etching with phosphoric acid, rinsing with an air-water
spray, drying, rewetting the preparation, applying the primer, drying,
applying the adhesive resin, and light-curing.
Based on the current clinical evidence and the recommendations of manufacturers, SE
adhesive systems can be used successfully for
the restoration of Classes 1, 2, 3, and 5 preparations. SE adhesives
provide adequate enamel etching to resist microleakage and marginal
staining and adequate retention of both prepared teeth and NCCL Class 5
restorations.
With the introduction of clinically reliable
self-etching bonding systems for use in the restoration of routine tooth
preparations, the practitioner can place restorations in a more simplified manner. SE systems are different from the bonding
systems previously used and the manufacturers recommendations must
be followed to ensure clinical success.
DISCLOSURE
The author has received honorarium or grant/research
support from 3M ESPE, Bisco, Den-Mat, DENTSPLY,
GC America, Heraeus Kulzer, Pulpdent, and
Ultradent.
REFERENCES
1. Leinfelder
KF, Kurdziolek SM. Self-etching bonding agents. Compend Contin Educ
Dent. 2003;24(6):447-456.
2. Buonocore
MG. A simple method of increasing the adhesion of acrylic filling materials
to enamel surfaces. J Dent Res. 1955; 34(6):849-853.
3. Cueto EI, Buonocore MG. Sealing of pits
and fissures with an adhesive resin: its use in
caries prevention. J Am Dent Assoc. 1967;75(1):121-128.
4. Torney DL, Denehy GE, Teixeira LD. The
acid etch class III composite resin restoration. J Prosthet Dent. 1977;38(6):
623-626.
5. Jordan RE, Suzuki M, Gwinnett AJ, et
al. Restoration of fractured and hypoplastic incisors by the acid
etch resin technique: a three year report. J Am Dent Assoc. 1977;95(4):
795-803.
6. Strassler HE. Applications of
total-etch adhesive bonding. Compend Contin Educ Dent. 2003;24(6):
427-436.
7. Brudevold F, Buonocore M, Wileman W. A
report on a resin capable of bonding to human dentin surfaces. J Dent Res. 1956;35:
846-851.
8. Diamond A, Carrel R. The smear layer: a
review of restorative progress. J Pedod. 1984;8(3):219-226.
9. Retief DH, Gross JD, Bradley EL, et al.
Tensile bond strengths of dentin bonding agents to dentin. Dent Mater. 1986;2(2):
72-77.
10. Eliades GC, Caputo AA, Vougionklakis
GJ. Composition, wetting properties and bond strength with dentin of 6 new
dentin adhesives. Dent Mater. 1985;1(5):170-176.
11. Lee HL, Orlowski JA, Scheidt GC, et al.
Effects of acid etchants on dentin. J Dent Res. 1973;52(6):1228-1233.
12. Torney DL. The retentive ability of
acid-etched dentin. J Prosthet Dent. 1978;3(2):169-172.
13. Skinner EW, Phillips RW. The Science of
Dental Materials. 5th ed. Philadelphia, PA: WB Saunders Company;
1960;277.
14. Jennings RE, Ranly DM. Autoradiographic
studies of P32 penetration into enamel and dentin during acid etching. ASDC
J Dent Child. 1972;39(1):69-71.
15. Fusayama T, Nakamura
M, Kurosaki N, et al. Non-pressure adhesion of a new adhesive restorative
system. J Dent Res. 1979;58:1364-1370.
16. Bertolotti RL. Acid etching of dentin.
Quintessence Int. 1990;21:77-78.
17. Kanca J III. One-year evaluation of a
dentin-enamel bonding system. J Esthet Dent. 1990;2(4):100-103.
18. van Meerbeek B, Inoue S, Perdigao J, et
al. Enamel and dentin adhesion. In: Fundamentals
of Operative Dentistry a Contemporary Approach.
2nd edition. Summitt JB, Robbins JW, Schwartz RS, eds. Hanover Park, IL: Quintessence Books, 2001;178-235.
19. Christensen G. Update on adhesive
systems. CRA Newsletter. 2002;26(6)2.
20. Perdigao J, Geraldeli S, Hodges JS.
Total-etch versus self-etch adhesive effect on
postoperative sensitivity. J Am Dent Assoc. 2003;134(12):1621-1629.
21. Tay FR, Sano H, Carvalho R, et al. An
ultrastructural study of the influence of acidity on self-etching primers
and smear layer thickness on bonding to intact dentin. J Adhes Dent. 2000;2(2):
83-98.
22. Perdigao J, Lambrechts P, van Meerbeek
B, et al. Morphological field emissions- SEM study of the effect of six
phosphoric acid etching agents on human dentin. Dent Mater. 1996;12(4):
262-271.
23. Akpata ES, Behbehani J. Effect of
bonding systems on post-operative sensitivity from posterior composites. Am
J Dent. 2006;19(3):151-154.
24. Perdigao J, Anauate-Netto C, Carmo AR,
et al. The effect of adhesive and flowable composite on postoperative
sensitivity: 2-week results. Quintessence Int. 2004;35(10):777-784.
25. Unemori M, Matsuya Y, Akashi A, et al.
Self-etching adhesives and postoperative sensitivity. Am J Dent. 2004;17(3):
191-195.
26. Browning WD, Myers M, Downey M, et al.
Reduction in post-operative sensitivity: a community based study. J Dent
Res. 2006;85(Special Issue B): Abstract #1151.
27. Miller MB. Self-etching adhesives:
solving the sensitivity conundrum. Pract Proced Aesthet Dent. 2002;14(5):
406.
28. Lee R, Blank JT. Simplify bonding with
a single step: one component, no mixing. Contemporary Esthetics and
Restorative Practice. 2003;7(5):45-46.
29. Santini A, Ivanovic V, Ibbetson R, et
al. Influence of cavity configuration on microleakage around Class V
restorations bonded with seven self-etching adhesives. J Esthet Restor
Dent. 2004;16(2):128-136.
30. Kanca J. Improving bond strength through acid
etching of dentin and bonding to wet dentin surfaces. J Am Dent Assoc. 1996;123(9):
35-43.
31. Gwinnett
AJ. Moist versus dry dentin: it effect on shear bond strength. Am J Dent. 1992;5(3):127-129.
32. Finger WJ, Tani C. Effect of relative
humidity on bond strength of self-etching adhesives to dentin. J Adhes
Dent. 2002;4(4):277-282.
33. Turkun M, Turkun LS, Kalender A. Effect
of cavity disinfectants on the sealing ability of nonrinsing dentin-bonding
resins. Quintessence Int. 2004;35(6):469-476.
34. Elkhatib H,
Nakajima M, Hiraishi N, et al. Surface pH and bond strength of a self-etching primer/adhesive system to
intracoronal dentin after application of hydrogen peroxide bleach with
sodium perborate. Oper Dent. 2003;28(5):591-597.
35. Perdigao J,
Geraldeli S. Bonding characteristics of self-etching adhesives to intact
versus prepared enamel. J Esthet Restor Dent. 2003:5:32-42.
36. Brackett WW, Ito S, Nishitani Y, et al.
The microtensile bond strength of self-etching adhesives to ground enamel. Oper
Dent. 2006;31(3):332-337.
37. Di Hipolita V, de Goes MF, Carrilho MR,
et al. SEM evaluation of contemporary
self-etching primers applied to ground and unground enamel. J Adhes Dent. 2005;7(3):
203-211.
38. Aljubouri YD, Millette DT, Gilmour WH. Six and 12
months evaluation of a self-etching
primer versus two-stage etch and prime for orthodontic bonding: a
randomized clinical trial. Eur J Orthod. 2004;26(6):565-571.
39. Murfitt PG, Quick AN, Swain MV,
Herbison GP. A randomised clinical trial to investigate bond failure rates
using a self-etching primer. Eur J Orthod. 2006;28(5):444-449.
40. House K, Ireland AJ,
Sherriff M. An investigation into the use of a single component self-etching primer adhesive system for orthodontic bonding: a randomized
controlled clinical trial. J Orthod. 2006;33:38-44.
41. Kiremiti A, Yalcin F, Gokalp S. Bonding to enamel
and dentin using self-etching adhesive systems. Quintessence Int. 2004;35(4):367-370.
42. Tay FR, Pashley DH, King NM, et al.
Aggressiveness of self-etch adhesives on unground enamel. Oper Dent. 2004;29(3):
309-316.
43. Lopes GC, Marson FC, Vieira LC, et al.
Composite bond strength to enamel with self-etching primers. Oper Dent. 2004;29(4):
424-429.
44. Perdigao J, Gomes G, Lopes MM.
Influence of conditioning time on enamel adhesion. Quintessence Int. 2006;37(1):
35-41.
45. Christensen G. Self-etch primer (SEP)
adhesives update. CRA Newsletter. 2003;2(11/12):1-5.
46. van Meerbeek B, DeMunck J, Mattar D, et
al. Microtensile bond strengths of an etch and rinse and self-etch adhesive
to enamel and dentin as a function of surface treatment. Oper Dent. 2003;28(5):
647-660.
47. Shimada Y, Iwamoto N, Kawashima M, et
al. Shear bond strength of current adhesive systems to enamel, dentin, and
dentin-enamel junction region. Oper Dent. 2003;28(5):585-590.
48. Senawongse P, Sattabanasuk V, Shimada
Y, et al. Bond strengths of current adhesive systems on intact and ground
enamel. J Esthet Restor Dent. 2004;16(2):107-116.
49. Tani C, Finger WJ. Effect of smear
layer thickness on bond strength mediated by three all-in-one self-etching
priming adhesives. J Adhes Dent. 2002;4(4):283-289.
50. Akimoto N. Ten-year clinical evaluation
of self-etching primer system. J Dent Res. 2004;83(Special Issue A):
Abstract #249.
51. Swift EJ Jr, Heymann HO, Pereira PNF,
et al. Clinical evaluation of a two-component self-etching adhesive and
hybrid composite. J Dent Res. 2005;84(Special Issue A): Abstract
#1780.
52. Turkun LS.
24-month clinical performance of two self-etching adhesive systems. J Dent Res.
2005;84(Special Issue A): Abstract #1782.
53. Anauate-Netto C, Carmo AR, Perdigao J,
et al. Clinical performance of a self-etching adhesive at 18 months. J Dent
Res. 2005;84(Special Issue A): Abstract #1783.
54. Burrow M. Five-year clinical evaluation
of One-Up Bond F in NCCL. J Dent Res. 2006;85(Special Issue B):
Abstract #1153.
55. Sergent R, Burgess JO, Gallo J, et al.
In vivo evaluation of two self-etching
adhesives, twelve month results. J Dent Res. 2006;85(Special Issue A): Abstract #351.
56. Pereira PNR, Swift EJ, Heymann HO, et
al. Clinical evaluation of a self-etching adhesive and a flowable
composite. J Dent Res. 2006;85(Special Issue A): Abstract #352.
57. Swift EJ Jr, Heymann H, Pereira P, et
al. Clinical evaluation of a two-component self-etch adhesive and
microhybrid composite. J Dent Res. 2006;85(Special Issue A): Abstract
#355.
58. Dunn J, Munoz C, Wilson AC, et al.
One-year clinical evaluation of Xeno IV in cervical lesions. J Dent Res.
2006;85(Special Issue A): Abstract #356.
59. Malmstrom H. 18 months clinical
evaluation of a self-etch bonding agent. J Dent Res. 2006;85(Special
Issue B): Abstract #641.
60. Hanabusa M, Akimoto N, Momi Y. One-year
clinical evaluation of one-step self-etching systems. J Dent Res. 2006;85(Special
Issue B): Abstract #1149.
61. Dalton Bittencourt D, Ezecelevski IG,
Reis A, et al. An 18 months evaluation of self-etch and etch &
rinse adhesive in non-carious cervical lesions. Acta Odontol Scand. 2005;63:
173-178.
62. Dunn JR. iBond. The seventh generation,
one-bottle dental bonding agent. Compend Contin Educ Dent. 2003;24(2
Suppl):14-18.
63. Tay FR, Pashley DH, Peters MC. Adhesive
permeability affects composite coupling to dentin treated with a self-etch
adhesive. Oper Dent. 2003;28(5):610-621.
64. Hillam R, Pasciuta M, Cobb D. Shear
bond strength of primer/adhesives with proprietary dual cure resin cement. J
Dent Res. 2002;81(Special Issue A):A-72, Abstract #369.
65. Pasciuta M, Cobb D, Denehy G. Shear
bond strength of dual cure primer/adhesives with dual cure resin cements. J
Dent Res. 2002;81(Special Issue A):A-76, Abstract #405.
66. Christensen G. Self-etch primer (SEP)
adhesives update. CRA Newsletter. 2003;27(11/12):1-5.
67. Cheony C,
King NM, Pashley DH, et al. Incompatibility of self-etch adhesives with
chemical/dual cured composites: two step vs one step systems. Oper Dent. 2003;28:
747-755.
68. Tay FR,
Pashley DH, Yiu CK, et al. Factors contributing to the incompatibility
between simplified-step adhesives and chemically cured or dual-cured
composites. Part 1. Single step self-etching adhesive. J Adhes Dent. 2003;5(1):
27-40.
|
|
|
| Figure 1A Class 2 carious lesion on the distal surface of the mandibular second premolar. |
|
Figure 1B Class 2 cavity preparation. |
|
|
|
| Figure 1C Restoration using a self-etch adhesive with a micromatrix hybrid composite resin. |
|
Figure 2A Class 3 carious lesion on the mesial surface of the maxillary lateral incisor. |
|
|
|
| Figure 2B Class 3 and lingual cavity preparations. |
|
Figure 2C Restorations using a self-etch adhesive with a microfill hybrid composite resin. |









{kind=link}
{kind=link}